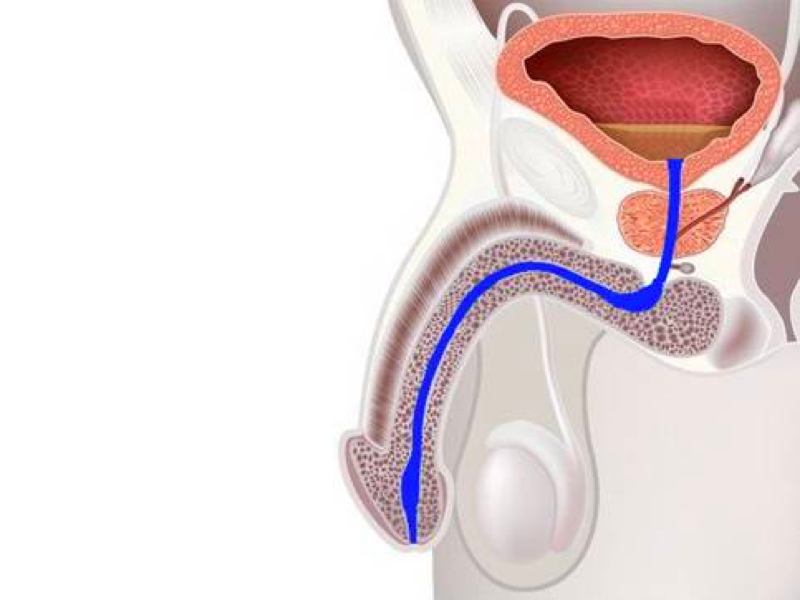







The urethra, which is narrow in closed surgery with a cold knife, is cut at 12 o’clock and opened and placed at the end. The process is simple. It ends in 15 – 20 minutes. The success rate is low.

In Laser Uretrotomy, the same process is performed with laser energy .
Is it cold knife or laser? In fact, there is no difference in success rates. It happens with both. It is the character of the stricture that determines success.

In this technique, the narrow urethra is cut and thrown, and the healthy urethra ends are sewn together.
Patch-style surgeries that expand the urethra : These surgeries can be performed in all urinary tract stenosis (shortest to longest). It is done using the hairless skin of the penis or the oral mucosa.

In this technique, the narrow urethra is not removed, it is drawn across and a patch is added to the floor or ceiling of the urethra.
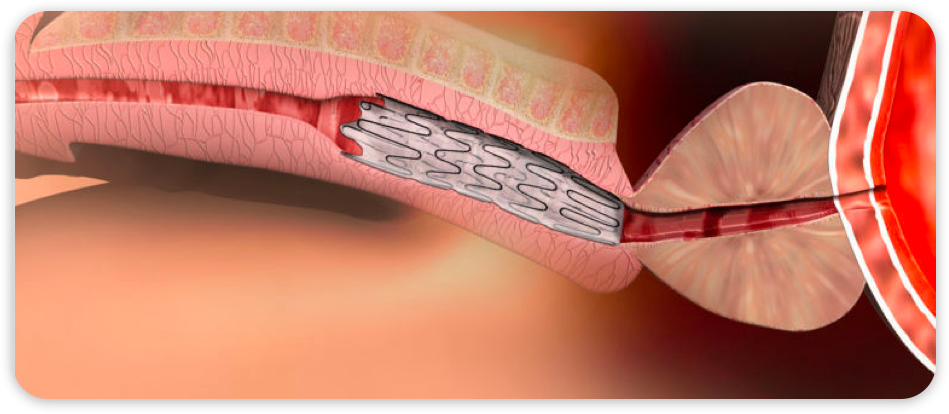
What do you think about urethra stents?
It should only be applied in very few patient groups. It should be used in patients who want to keep the urinary tract open in a short and simple way, with the elderly short-lived. Patients who have had permanent stents in the past travel around in the middle as a urethra injury. In 7 such patients, we had surgeries that removed the stent and repaired the urinary canal, and we were successful in all of them.
When can I go to work?
Normally, work starts after 1 week. However, since catheter removal time can be up to 3 weeks, the catheter can be returned to work.