
Urogenital System Traumas
Only 10% of all body traumas concern the urogenital system. Emergency physicians, traumatologists, and general surgeons perform the first response to a patient with general body trauma in the emergency unit of the hospital. Urologists are often invited as consultant physicians. Therefore, vital functions of these patients are supported. The vascular access and airway are kept open. Combat with hemorrhage and shock table. If necessary, resuscitation is performed. A detailed history is taken. The form of the trauma, its time, and the parts of the body where trauma is effective are determined. In the urological examination; In the lumbar region, the findings that may be related to the cutting tool and blunt injury are noted. The presence of globe vesica, genital examination, blood is checked for urethral meatus. If there is no blood, it is attempted to gently push a urethral catheter into the bladder. If the catheter does not pass, no force is applied and a suprapubic cystostomy catheter is inserted. Next, advanced radiological imaging methods are used to illuminate the basic pathology.
Bladder Traumas
Bladder injuries can be due to blunt, penetrating or iatrogenic causes. However, only 2% of intra- abdominal emergency pathologies requiring surgical repair are bladder injuries. This is because the bladder is a hollow organ and the bone is naturally protected by the pelvis. 67-86% of bladder injuries are blunt and 14-33% penetrating. The most common cause of blunt trauma is motor vehicle accidents with a full bladder. If urine leakage occurs immediately around the bladder, it is called extraperitoneal rupture, if it is inside the peritoneum, it is called intraperitoneal rupture.
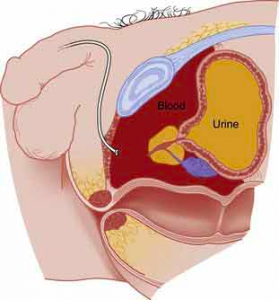
After blunt bladder injury, the urinary canal is broken, the bladder and prostate have escaped, the cavity is filled with blood (burgundy). 70-97% of blunt bladder trauma is with pelvic fractures. These; The symphysis pubis and sacroiliac joint separations are in the form of sacral, iliac and pubic bone fractures. Bladder injuries can also occur without a bone fracture. These injuries are usually blunt injuries or seat belt injuries on the full bladder. Bladder injuries; It was divided into five groups by Sandler and his friends.
Bladder Injury Classification
1 Bladder contusion
2 İntraperitoneal rupture
3 İnterstitial bladder injury
4 Extraperitoneal rupture ( A: Simple, B: Complex )
5 Combined injury
Diagnosis
Macroscopic hematuria (82%) and abdominal tenderness (62%) are the most common symptoms and signs in patients with major bladder injury. Other findings; There may be different findings depending on the area of urination, suprapubic ecchymosis, abdominal distension and urinary extravasation.
Macroscopic hematuria
It is definitely a finding of trauma in a patient who did not have macroscopic hematuria before. Morey et al. Detected macroscopic hematuria in all patients with bladder rupture, and reported that 85% of these were accompanied by pelvic fracture. Therefore, it is strongly recommended to perform cystography in patients with pelvic fractures and hematuria together.
If a traumatized patient does not have a pelvic fracture and the urine is clear, there is most likely no bladder trauma. However, it should be noted that bladder injuries may occur in 2-10% of these cases. In a retrospective study involving eight thousand patients, Tarman et al. Detected extraperitoneal bladder rupture in only 05% of cases with pelvic fracture and reported that further investigation is not required if there is no macroscopic hematuria.
Microscopic hematuria
There is no consensus in the literature on whether or not a further investigation is required in which patient group. In some studies, it was reported that bladder rupture was not observed in each field when there were less than 25 erythrocytes. However, in the final decision making, the general condition of the patient and the observation and examination findings of the physician are important.
Cystography
It is the standard and most sensitive diagnostic procedure in the evaluation of bladder trauma. If the bladder is sufficiently filled and if post-voiding images are taken, accurate diagnosis is achieved by cystography at the rate of 85-100%. Contrast overflows outside the bladder is pathognomonic. During the procedure, plain film, half full, full and empty bladder images should be taken after contrast, and oblique images should be added in necessary cases. 10% of bladder ruptures are detected only on empty bladder images

Fracture in the ischium arms and contrast coming out of the bladder in cystography

Break in the bladder neck, rising of the bladder towards the cranial, perivesical contrast accumulation in the pelvis (Long arrows: raised bladder, Short arrows: contrast extravasation)
Intravenous pyelography (IVP)
Since the contrast is diluted and the bladder pressure is low during the procedure, it is insufficient to show minor bladder injuries. IVP can only help in 15-25% of patients. It shows false negativity in 64-84% of patients. Therefore, it is not recommended in the diagnosis of bladder injuries.
Ultrasonography
It has no place in routine use. However, it can provide information about the location and amount of extravasation. It can give an idea about bladder injury indirectly by showing that the fluid sent from the urethra during the ultrasonography does not pass into the bladder.
Computed tomography (CT)CT is the method of choice for the evaluation of patients with blunt and penetrating abdominal and / or pelvic trauma. CT shows intraperitoneal and extraperitoneal fluid but cannot separate urine from acid. In a series of 316 patients, Deck et al. Diagnosed bladder rupture in 44 cases and reported that the CT findings in these cases were 82% correlated. In conclusion, CT cystographic findings have been found effective in the accurate detection of bladder damage, and it has been emphasized that it is effective in directing treatment with less radiation exposure than conventional cystography and without additional costs.
Angiography
It is a rarely used method and it is used to reveal a hidden bleeding focus and embolization when necessary.
Magnetic Resonance Imaging (MRI)
It is not recommended in the acute period of trauma.
Cystoscopy
It is not recommended since an optimal image cannot be achieved due to bleeding.
Differential diagnosis
Differential diagnosis in a patient with macroscopic hematuria; It should be done with kidney, ureter and urethra injuries.
Treatment
First, the patient is expected to stabilize. Treatment of bladder injury is started after life-threatening situations are resolved. Steps to be taken respectively in treatment are shown below.
Blunt trauma: Extraperitoneal rupture
Most patients with extraperitoneal rupture can only be treated with catheter drainage, even in the presence of extensive retroperitoneal or scrotal extravasation. Obstruction of the catheter with clots or tissue debris can prevent timely healing. Cass and Luxenberg reported a 93% success rate with this approach in a series of 30 patients with extraperitoneal rupture. 87% of the ruptures healed within 10 days, all within three weeks. However, surgical intervention is necessary in the presence of bladder neck involvement and bone fragments in the bladder wall or if the bladder wall is injured in person.
Blunt trauma: Intraperitoneal rupture
Intraperitoneal ruptures occurring after blunt trauma should always be treated with surgical exploration. Due to the severity of the damage caused by this type of damage, it carries a high mortality rate of 20-40%. In these cases, lacerations are generally large and if left untreated there is a risk of peritonitis due to urine leakage. Abdominal organs should be examined for possible damage and urinoma should be drained.
Penetrating damage
Emergency exploration and repair should be performed in all bladder perforations due to penetrating trauma.
Complications
If pelvic hematoma or urinary extravasation is infected, pelvic abscess may develop. In intraperitoneal bladder ruptures, the passage of urine into the abdominal cavity can lead to a delayed peritonitis. An injury to the bladder neck can cause partial incontinence.
Prognosis
If it is treated appropriately and on time, the prognosis is excellent. The cystostomy catheter is removed on the tenth day if the patient is functioning normally.
PNL (Percutaneous stone surgery)
The stone in the kidney is reached by entering a pen-thick hole from the back of the patient lying prone in the operating room, and the stone is broken and the pieces are taken out. It may take 1-3 hours. He is hospitalized for 1 day. 80-90% of the stone is saved. Please click the link for the surgery video.
RIRS (Entering through the Urinary Canal, breaking the kidney stones with laser)
This method has become popular in recent years. It is done in the operating room. By entering through the natural cavities of the body (urinary canal), the kidney is reached and the stones are broken into powder under direct vision with holmium laser. The patient spills his own stones and is sometimes collected by the physician. The process may take 1-3 hours. Stents can be placed during the procedure. He is hospitalized for 1 day and discharged.
Open Surgery:
It is rarely done today. Open surgery may be an option if there is urinary tract stenosis that requires repair together or if the stone fills the entire kidney.
Which method is better?
The most important factor that determines this is the possibilities at hand, the experience of the urologist, the patient’s expectation and cost. The cheapest method is the ESWL method. The chance of getting rid of the stone varies between 30 and 100%. Requires session. There is no guarantee of exact breaking. Even if it is broken, the stone may not fall. It may require a secondary surgery. The PNL (surgical technique through the hole through the back) gives very good results in suitable patients. It can be completely removed from the stone. However, if the stones are very scattered, the patient may remain in the stone after the procedure. These remaining stones can be broken with ESWL. RIRS, that is, entering the urinary canal, and breaking the stone with laser does not disrupt body integrity, has become popular today. Surgery is performed by entering through the urinary canal. It is the first treatment considered in patients with bleeding problems.
How do we do it?
First of all, we reveal the stones of the patient with the most modern imaging methods. We consider the surgeries it has undergone and the applications it has undergone. We question the patient’s expectations, profession, lifestyle, and we determine the most appropriate method for that patient. We have the opportunity to apply all modern techniques applied to stone in the world.
Life Style Advice
2.5 lt of water should be drunk daily for life. Diet should be observed. An active life should be chosen. It should not sweat excessively. Regular checks should be made. It should be fed a diet that is poor in oxalate.