Urine Leakage From Bladder to Kidney
How Many Kinds and Which Diseases are Associated with Reflux (Urine Leakage)?
The most common type is the weak congenital bladder muscle (Figure 1). In addition, some children have two ureters (urinary tract). In some children, there are cases when the urinary canal, which we call ureterocele, buds inside the bladder like a cobra head. These children are candidates for urine escape from the bladder to the kidney. In one of the kidney diseases, which we call multicystic dysplastic kidney, 20-40% reflux can be seen in the opposite kidney. In addition, a 50% reflux can be seen in these patients due to posterior urethralvalv, an innate stenosis in the urinary outlet of boys. Apart from the congenital diseases mentioned above, reflux related to the following diseases can be seen;

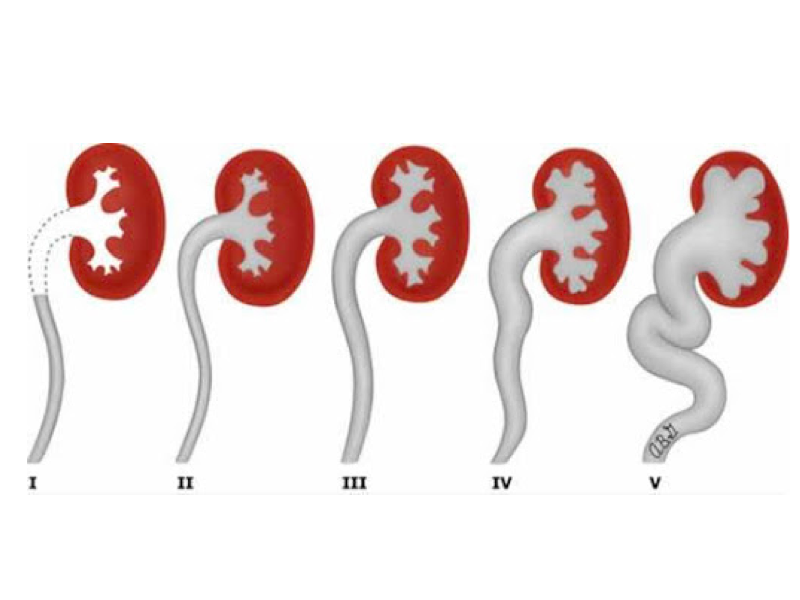
Escape from I – V Bladder to Kidney is evaluated in 5 categories. Indicates I (light), II-III (Medium), IV-V (Advanced Level) Reflection.
A- Reduced Bladder Capacity
When the bladder capacity is small, the ureterovesical junction (valve) may deteriorate due to high pressure over time, causing a secondary reflux.
B- Intestinal Bladder Dysfunction
This situation is very important. Sometimes only the treatment of an underlying hidden constipation treats the disease.
C- Prune-Belly Syndrome
A group of congenital diseases characterized by weakness of the abdominal muscles.
Can We Rate Reflux Disease?
Yes, we can divide this disease to 5 degrees according to the level of urine leakage and deformation in collector system. While the 1st degree leaks only to the ureter, the 5th grade leaks up to the calyx of the kidney, and some deterioration has started in the collector system.
What kind of troubles can be encountered if reflux is not treated?
Recurrent urinary tract infections can occur and kidney function losses occur with each infection. These losses cause irreversible damage to the kidney. The higher the degree of leakage, the higher the level of damage seen over time. As a result of this damage, kidney function may completely lose and blood pressure can be added to the disease.
What findings do vesicoureteral reflux give?
In fact, an enlargement of the kidney can be seen by ultrasonography during the controls performed in the womb before delivery. The first finding after birth may be a urinary tract infection. It is usually diagnosed at the ages of 3-6. It is seen in 85% of girls. It is observed in men at an earlier age, to a higher degree, and often with voiding problems.
What methods are available for diagnosis?
In the first stage, urine analysis, urine culture and ultrasonography are performed. If reflux is suspected, DMSA scintigraphy is performed to understand the state of kidney function. For definitive diagnosis, voiding cystography (Figure-3) is performed. For this purpose, a substance is given to the bladder to see if there is a leak. This method can also be done with agents used in nuclear medicine. In addition, some extra examinations are carried out to rule out situations that may interfere or increase leakage. Another issue to remember is that kidney tests are performed in bilateral reflux and single kidney patients.

Imaging of the leak with the drug given through the urinary tract. We see it at 5 degrees in the figure.
If one of the children has reflux (leakage of urine), can it be seen in others? Also, Are There Any Other Risks To Be Diagnosed Early?
The probability of being seen in siblings is 27%. If the mother or father has reflux disease, the probability of being seen in the child is 36%. If a baby has an enlarged kidney in the ultrasound performed while in the womb, there is a 15% chance of reflux in this baby. In babies with these risks, some tests should be done early and precautions should be taken.
Is there any possibility of self-healing of reflux?
Yes, this possibility is considerably high. However, its diagnosis and degree should be established and factors that may cause an increase in discomfort should be eliminated. If the degree of reflux is high, bilateral, intestinal disorders, or other abnormalities in the urinary tract, there is a possibility of spontaneous recovery. During this waiting period, some medications should be used. However, it should not be forgotten that 30% of the self-regressing reflux progresses over time.
What is the Main Purpose in Reflux Treatment?
Our main goal is to prevent recurrent urinary tract infections and protect the kidney. For this purpose, if there is a cause such as urethral stenosis, posteriorurethral valve, voiding disorders, intestinal problems, it is treated first.
Do You Prefer the Medicine in Reflux Treatment or Surgery?
There are many criteria that we consider when making this choice. For example, in patients with advanced reflux, antibiotics alone may not be sufficient for protective purposes. It is important for the patient age. In patients under 1 year old, we only provide antibiotic treatment if necessary. We do not prefer surgery in this age group.
Would you recommend circumcision to the patient who was followed for reflux?
Yes, I would definitely recommend it because it reduces the risk of infection.
What are the Surgical Treatment Options?
If the patient’s age is too young, a simple procedure can be performed to facilitate urine output, which we call cystostomy only. The aim here is that the kidneys are not damaged until they can be operated. Another surgical treatment option is drug administration (subureteric injection) to prevent the leakage of urine into the mouth of the canal with reflux (Figure 4-5). Especially in those with low reflux, the results are satisfying.


